Pilot model presented to Alabama task force shows high adherence and reported cost avoidance
Get AI-powered insights, summaries, and transcripts
Subscribe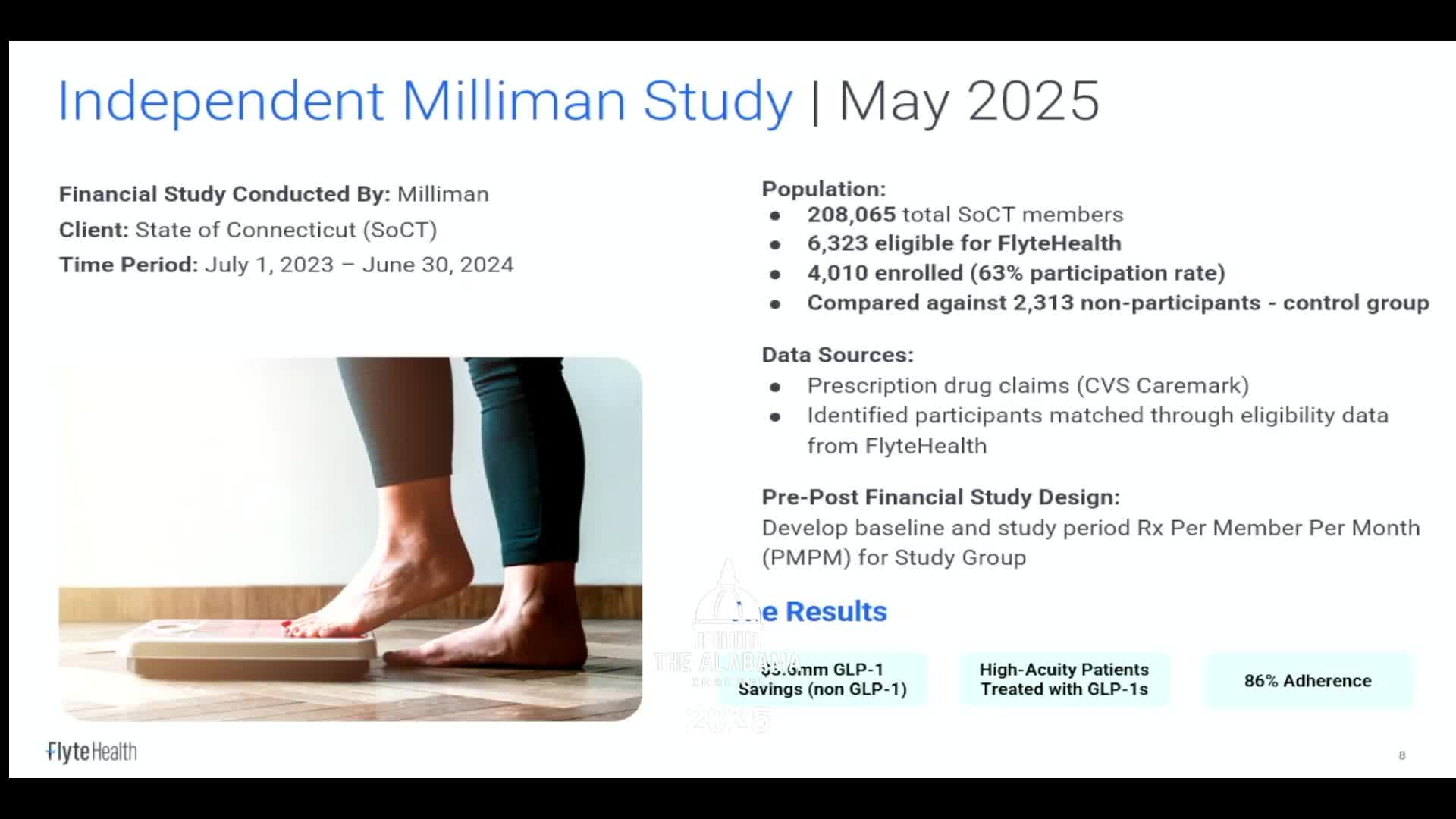
Summary
Dr. Saunders described a closed‑network, acuity‑based pilot run for a Connecticut state employee health program that reportedly achieved 86% adherence among about 4,000 participants and roughly $3,000,000 in annualized cost avoidance; she cautioned two‑year data are preliminary and implementation details matter for generalizability.
Dr. R. Saunders presented results from a closed network, acuity‑based program her group ran with the state of Connecticut, which she said was piloted in 2023. Saunders said the pilot initially managed several thousand patients who were already on medications and that the program focused on matching medication intensity to medical complexity and providing comprehensive wraparound services.
Saunders cited a one‑year analysis by the actuarial firm Milliman that compared about 4,000 program participants to non‑participants, reporting an 86% adherence rate and more than $3,000,000 in annualized cost avoidance. "Our adherence rate was 86 percent," she said. She attributed the result to intensive front‑end evaluation, coordination with specialists, stepwise medication strategies, and use of technology for ongoing monitoring.
Saunders said two‑year results exist but were not yet shareable in full. She emphasized that the model used a limited closed network at first to prove outcomes and then expanded provider training and partnerships (for example, with Emory) so systems could either refer to her group's program or adopt the trained model.
On limitations, Saunders warned that outcomes from a closed, specialist‑supported network with decision‑support tools may not immediately generalize to settings without training or ongoing monitoring. She recommended careful design of any scaled program, including gold‑carding trusted providers, aligning prior‑authorization to guideline‑based care, and ensuring long‑term maintenance programs.