Statewide Medicaid managed care starts; NVHA outlines network and oversight plans
Get AI-powered insights, summaries, and transcripts
Subscribe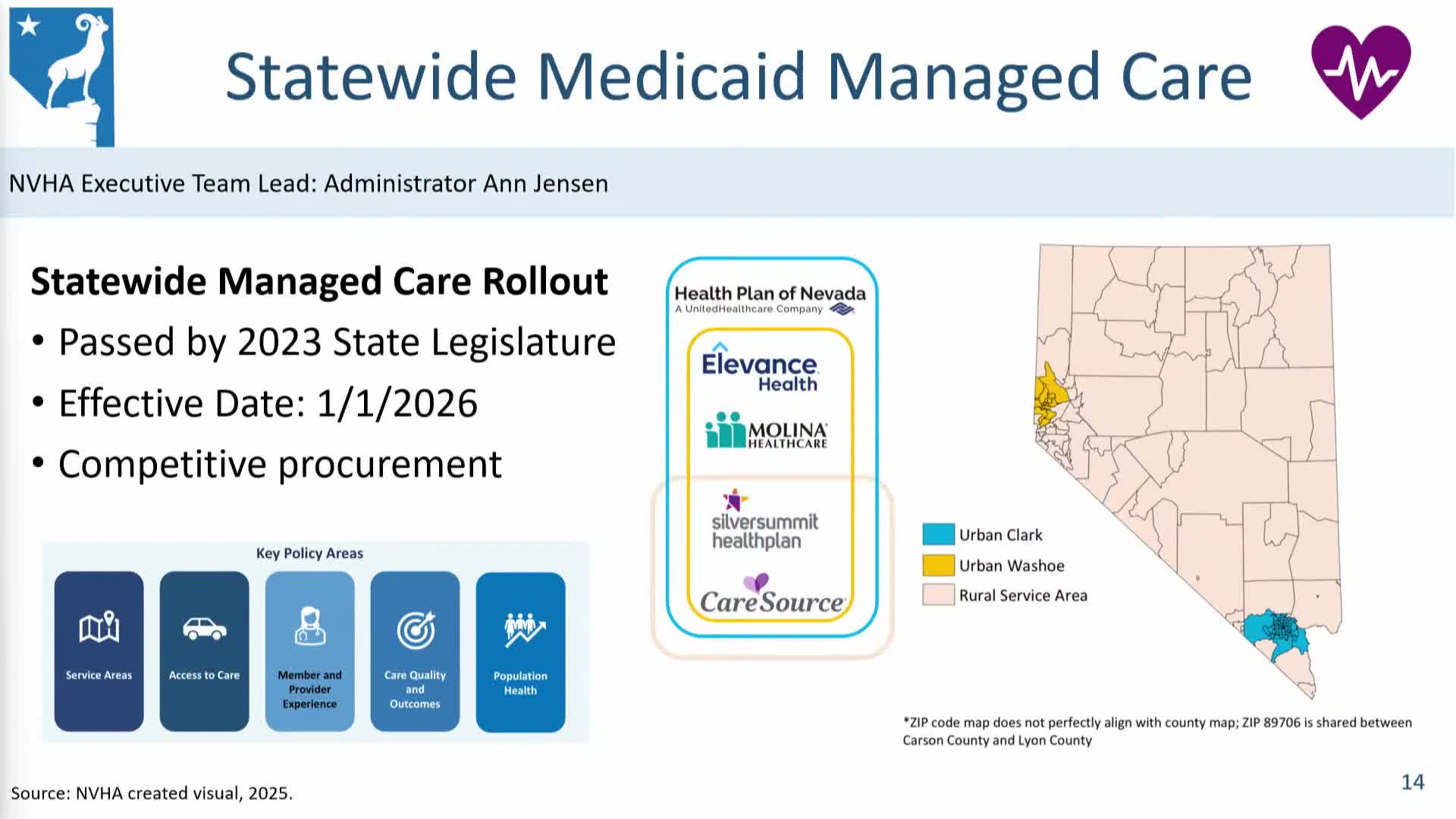
Summary
NVHA told lawmakers that statewide managed-care expansion began Jan. 1, with rural markets limited to two plan choices to preserve provider networks. Agency leaders said they met readiness reviews, will monitor network adequacy through an independent external review organization (HSAG) and will use contracting tools and quality withholds to hold managed care organizations accountable.
Nevada’s statewide Medicaid managed‑care rollout took effect Jan. 1, agency officials told the interim committee, expanding plans that had previously operated only in Clark and Washoe counties into rural service areas. Stacy Weeks said the procurement aimed to balance choice with network adequacy in rural counties by limiting the number of carrier contracts (two in some rural service areas) while providing more options in urban centers. "We picked our 2 top performers in rural," Weeks said, noting partners CareSource and Silver Summit Health Plan in rural regions and the addition of Health Plan of Nevada in Clark County.
Lawmakers questioned how the agency will monitor network adequacy, especially for new entrants such as CareSource. Weeks said NVHA uses an independent external review organization (HSAG) to monitor network adequacy and quality metrics under federal law, and that NVHA completed federally required readiness reviews before implementation. "We will use HSAG ... to monitor progress," she said.
NVHA described several contract levers to improve quality: value‑based payment design, required community reinvestment and a quality collaborative focused initially on hospitals and maternal health. Anne Jensen, Nevada Medicaid administrator, said the agency will use contractual quality withholds and regular monitoring to incentivize improvements, but acknowledged that improving star ratings often requires tying financial incentives to performance.
Members urged careful monitoring in rural areas and asked for early demographic and enrollment data; NVHA said it is sharing demographic rollup information with committee members and will provide further reports as enrollment stabilizes. Agency officials also noted protections for certain providers (directed payments for critical access hospitals) to preserve cash flow and access in sparsely populated counties.