Senate Health & Welfare reviews 12-page inventory of incoming reports, flags missing filings and overlaps
Get AI-powered insights, summaries, and transcripts
Sign Up Free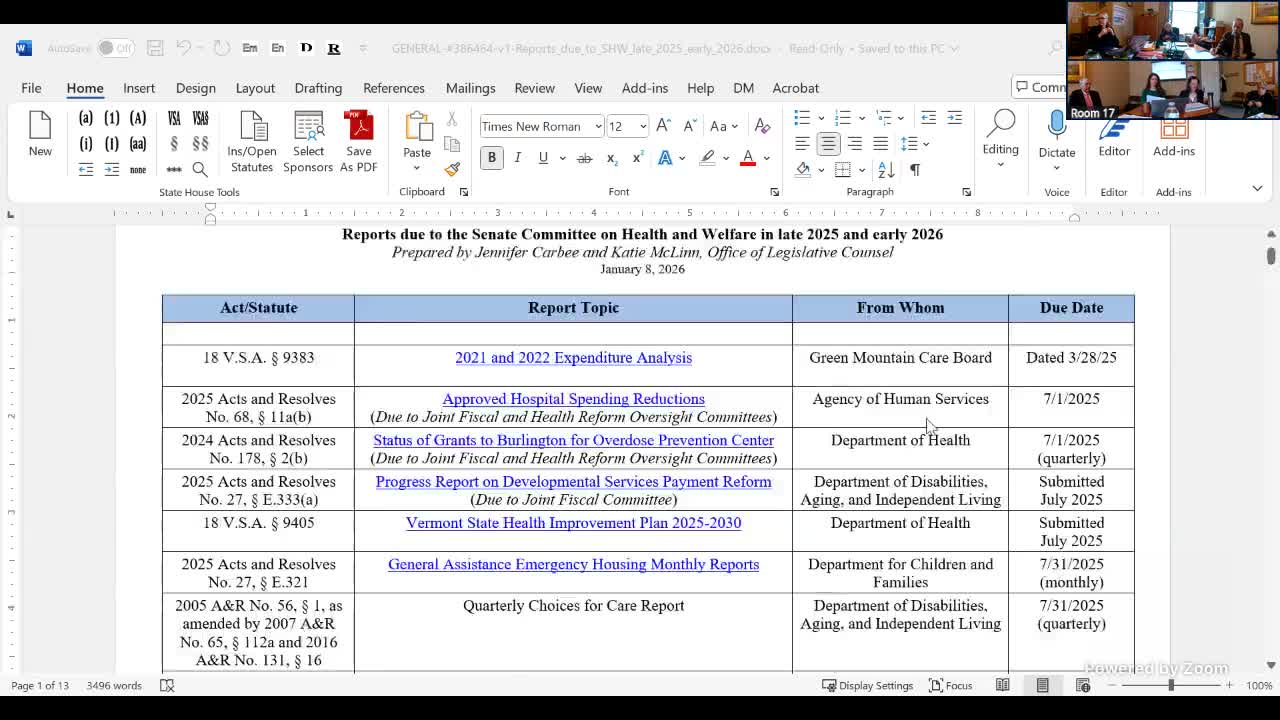
Summary
Senate Health & Welfare staff reviewed a 12-page list of reports due to the committee on Jan. 8, flagged multiple missing or inconsistently filed items (including a Choices for Care quarterly report), and asked members to prioritize which recurring reports warrant continued oversight.
On Jan. 8, the Vermont Senate Health & Welfare committee reviewed a compiled inventory of reports due to the committee and asked staff to help prioritize which items require continued oversight. Staff from the Office of Legislative Council — John Carvey and Katie McLennan — presented the list and links to posted reports.
The inventory included one-time and recurring reports across health programs. Staff highlighted an expenditure analysis from the Green Mountain Care Board covering 2021–2022 that the board produced after a methodology overhaul, and multiple Act 68 reports on hospital spending reductions and outcome measures for health care transformation. Unidentified Speaker 3 described recurring quarterly updates on the Burlington Overdose Prevention Center, noting earlier filings said the city council had approved the center and that work was under way on insurance coverage.
Committee members raised two recurring themes: missing or late postings and the overall volume of reporting. Staff said the Department of Disabilities, Aging and Independent Living may need to resubmit a quarterly Choices for Care utilization/expenditure report because it could not be found on the legislature’s website. Unidentified Speaker 1 said, “I don't know why we need a report on deaths and hospice,” and pushed the committee to identify which reports are critically important and which might be discontinued or referred to Government Operations for consolidation.
The inventory also flagged several items with fiscal implications or concrete figures: the hospital transformation incentive grant update (staff noted $2,000,000 was appropriated for incentive grants, with the agency asked to report on obligations as of Nov. 14); a University of Vermont network settlement the transcript estimates at about $11,000,000 and committee interest in how those funds will be distributed to non-network primary care providers; and $10,000,000 in Medicaid provider stabilization grant funds from last year’s budget, for which the administering department must report recipients and outcomes.
Other reports listed included the Green Mountain Care Board annual bill-back report (statutory bill-back of regulatory costs), an annual Global Commitment investment list tied to the Section 1115 demonstration, a hospice deaths report for FY22–23, a DFR (Department of Financial Regulation) Act 68 review of insurer sustainability (including Blue Cross Blue Shield of Vermont), an early education implementation plan and related child-care workforce items, an inventory of recovery residences, and a one-time review of a Medicaid payment model for residential substance use disorder treatment required by Act 3.
No formal motions or votes occurred; the meeting concluded with the chair (Unidentified Speaker 1) asking members to review the 12 pages of reports, check off items they want to retain or question, and return with staff (including Katie McLennan) to walk through the list in detail at a subsequent meeting.
Why it matters: the packet contains recurring monthly and quarterly filings required for legislative oversight of health programs and major funding streams. Committee members signaled a desire to reduce redundancy and focus oversight resources where the reporting yields material insight into program performance, fiscal exposure, or compliance with statutory requirements.
Next steps: members were asked to mark reports they view as critical or not needed and to reconvene with staff to determine which reports to continue receiving, which to recommend for consolidation, and which missing reports need resubmission or follow-up.