Lifetime Citizen Portal Access — AI Briefings, Alerts & Unlimited Follows
OHA and CCOs describe surge in behavioral health utilization and tighter federal scrutiny of directed payments
Loading...
Summary
Oregon Health Authority and CCO representatives said directed payments that began in 2023 increased outpatient capacity but also drove utilization beyond expected revenue, producing multi-hundred-million-dollar shortfalls for some coordinated care organizations and prompting narrower 2026 targeting amid heightened federal review.
Oregon Health Authority presenters and coordinated care organizations told the House Interim Committee on Behavioral Health that policy changes that boosted behavioral health capacity also produced rapid increases in service utilization that now strain CCO finances.
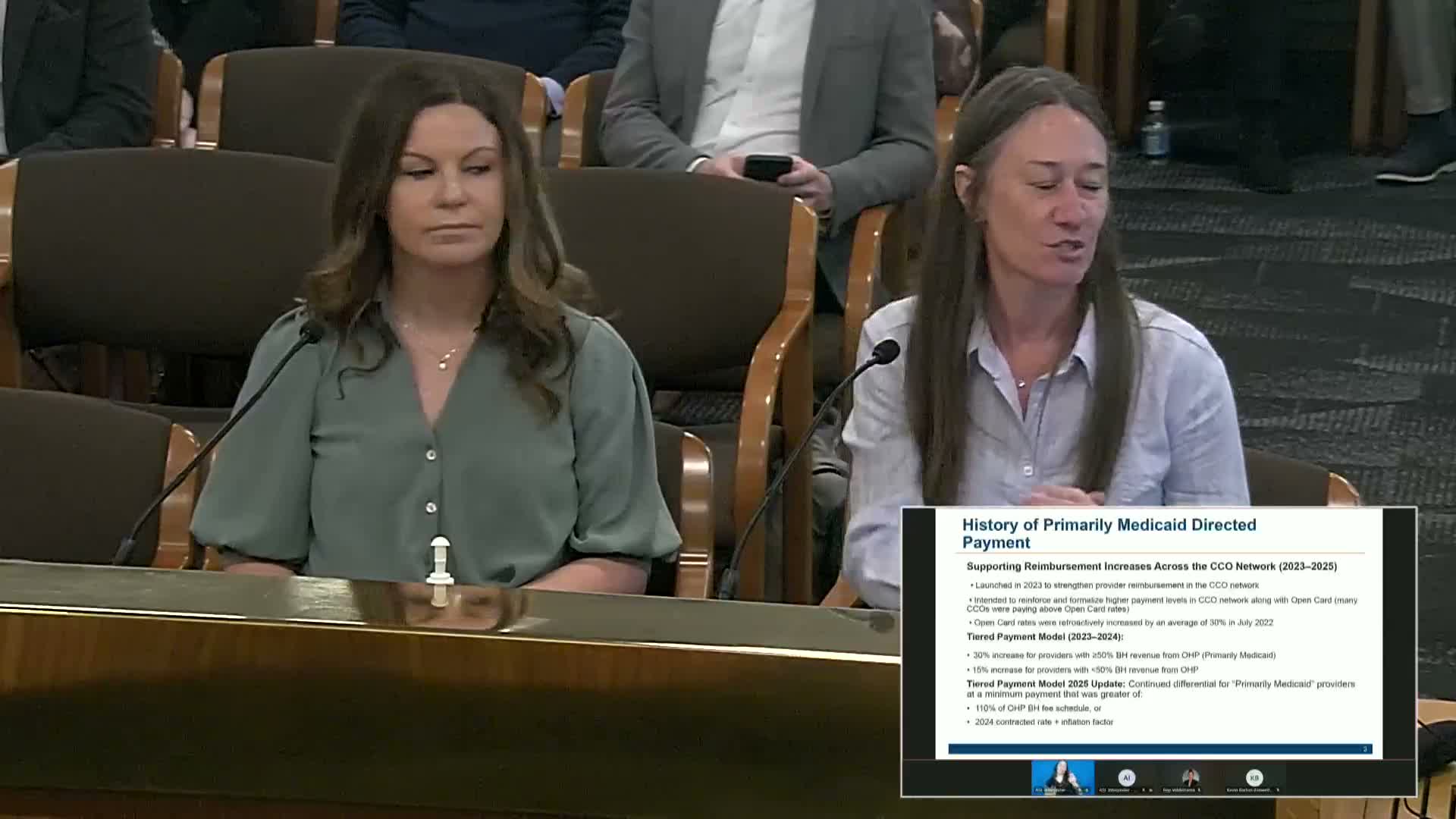
Chelsea Guest, CCO finance director at OHA, described how directed payments (begun in 2023 after a major legislative funding increase) were designed to ensure rate increases flowed to providers. She said the program’s design evolved and that the 2026 concept narrows eligibility so CCOs prioritize higher payments for providers who serve the most acutely ill Medicaid members and already deliver team-based care.
Guest said federal oversight of directed payments has tightened: "Directed payments are coming under very tight scrutiny from the federal government… We’re seeing stricter reviews, delays and approvals," and that some states are moving away from directed payments or adding caps.
Representatives of CCOs described operational strain. Jeremiah Rigsby of CareOregon said the combination of utilization increases and lagging revenue produced deep losses—CareOregon reported heavy financial losses across 2023–24 and estimated continuing deficits—while PacificSource described large-scale contract renegotiations to align provider payments with new criteria. EOCCO noted that high Medicaid reimbursements in some rural counties have attracted providers focused on lower-acuity therapy services and that the shift complicates sustaining a safety-net provider infrastructure.
Panelists and committee members discussed possible responses including improved rate-setting processes, negotiating value- and access-based contracts, and narrowly targeting directed payments to preserve resources for higher-acuity care. OHA said CCOs remain responsible for negotiating contracts and monitoring networks, and that 2026 rules intend to give CCOs more flexibility to direct limited funds to where they can serve highest-need Medicaid members.