AHS highlights $9.9M in program reductions and cuts loan‑repayment and legal‑aid contracts, drawing committee concern about workforce gaps
Get AI-powered insights, summaries, and transcripts
Subscribe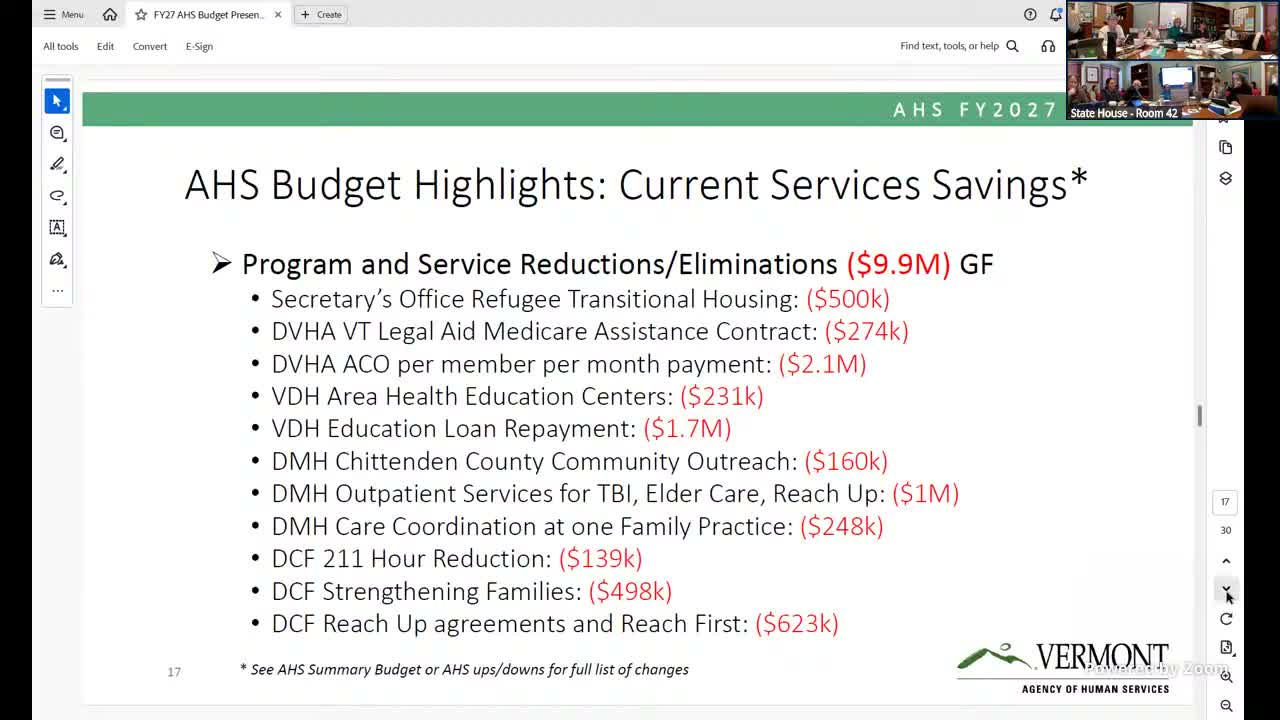
Summary
AHS told legislators it identified roughly $9.9 million in program reductions, including cuts to refugee transitional housing, an AHEC loan‑repayment program and a Vermont Legal Aid Medicare assistance contract; committee members pressed for data on impacts and worried about workforce consequences.
Agency of Human Services officials told the committee Feb. 5 that they identified about 38 program reductions and eliminations, totaling about $9.9 million in general‑fund savings, and said those cuts were part of a broader effort to reconcile agency needs with available targets.
Secretary Jenny Samuelson said the reductions were made collectively by the executive leadership team after reviewing program performance, duplication and statutory constraints. "These were very difficult decisions that we didn't take lightly," she said.
Several highlighted reductions and implications:
- Refugee transitional housing: AHS said a $900,000 base allocation had been built previously but projected refugee arrivals have fallen by about 75%, so $400,000 would remain to support limited transitional housing and case management services. AHS presenters said the refugee program currently requires less base funding because fewer people are arriving in Vermont.
- Vermont Legal Aid Medicare assistance contract: AHS described a statutory requirement that the contract be cost‑efficient; presenters said current revenue from the program is substantially below its cost and that statute allows cancellation when it is not cost‑effective.
- AHEC loan‑repayment: AHEC's loan‑repayment program was proposed for elimination because AHS determined it overlapped with VSAC programming. Committee members warned that eliminating AHEC funding may leave trainees and early‑career providers with a funding gap and questioned whether rural health transformation funds can be stood up quickly enough to replace the benefit. AHS said the rural health transformation program will require rapid obligation of $195 million in the coming period and that some workforce investments under that program differ from guaranteed individual loan repayment.
Committee members repeatedly asked for supporting data. One member said, "We need to see that data for these programs," and asked AHS to provide written documentation of program performance and the assumed savings. AHS agreed to follow up with a condensed department‑by‑department summary and additional data for committee review.
Presenters acknowledged transitional impacts on trainees and providers but stressed that some workforce investments under rural transformation will be available; they also noted federal restrictions on how certain transformation funds can be used, depending on service geography.
The briefing closed with agency staff offering to return with more detailed slides and written analyses for committee consideration before budget decisions are finalized.