HCA says Medicaid reentry waiver is scaling up; dozens of county and DOC facilities to join July 1
Get AI-powered insights, summaries, and transcripts
Subscribe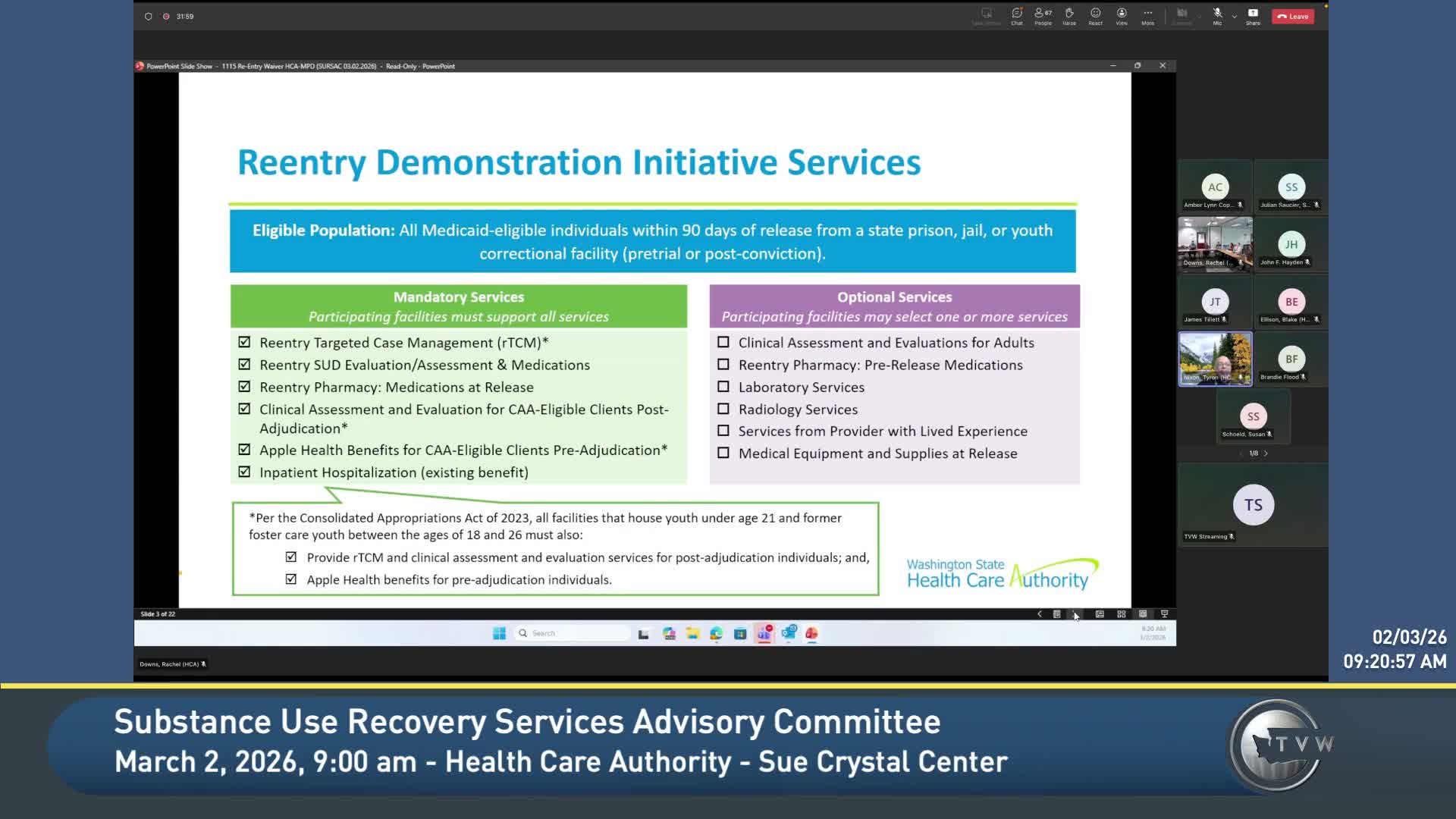
Summary
HCA told the advisory committee that Apple Health began covering targeted prerelease services in July 2025 and that cohorts of jails and juvenile facilities have launched; HCA expects many Department of Corrections sites and 15 additional facilities to join a July 1 cohort, while noting technical, contracting and billing challenges for some counties.
Tony Walton, chair of the Substance Use Recovery Services Advisory Committee, invited Tyree Nixon, transformation implementation manager at the Health Care Authority, to brief the committee on the reentry waiver and where it stands.
Nixon told the committee that Washington’s Apple Health started paying for a defined set of prerelease services beginning July 1, 2025, for Medicaid-eligible adults and youth who are incarcerated. "Beginning 07/01/2025 ... within 90 days of release, Washington State's Medicaid program or Apple Health will pay for a targeted set of prerelease services for Medicaid eligible adults and youth," Nixon said. The services include reentry-targeted case management, support for substance use disorder treatment, a 30-day supply of medication at release and clinical assessments required under the Consolidated Appropriations Act for some juveniles.
Nixon reviewed the program’s onboarding process and cohorts. He said 12 facilities launched in cohort 1 (eight on 07/01/2025 and four on 11/01/2025) including Spokane County juvenile facilities, Clallam County facilities, Kitsap County and others. Cohort 2 launched Jan. 1, 2026 (including South Correctional Entity and Walla Walla juvenile facilities). Cohort 2b included six facilities that went live the day before the meeting (Echo Glen and Green Hill among them), and Nixon said the program expects a larger cohort 3 on July 1 that will include Department of Corrections facilities such as Coyote Ridge, Clallam Bay, Washington Correction Center for Women, Cedar Creek, Stafford Creek, Monroe, Airway Heights, Washington State Penitentiary and Washington Correction Center.
Nixon described a readiness-assessment and milestone approach for onboarding. Participating facilities complete a capacity-building application, attest they can bill Medicaid, run reentry-targeted case management and support medication continuity, and take part in rapid-response calls with subject-matter experts (eligibility, pharmacy, provider enrollment, MCO representatives and DBHR staff). A third-party administrator (TPA) — Community Health Partners Services (a CHPW division named in the briefing) — assists with technical support and claims clearinghouse functions.
The presentation highlighted successes and practical challenges. Nixon said some facilities report early signs of reduced recidivism and new clinical linkages — for example, Nisqually cited fewer repeat incarcerations after services started. He also shared a concrete clinical outcome: some facilities secured hepatitis C medications for people in custody. At the same time, facilities have struggled with contract changes when initial community provider partners dropped their contracts, with electronic-health-record and firewall problems affecting information sharing, and with unfamiliar billing codes and claims workflows. "Facilities understanding what it takes to submit a claim and bill ... All of that is brand new," Nixon said.
Committee members asked whether telemedicine-only models used by some jails would meet program requirements. Nixon said that the waiver has mandatory elements — including warm handoffs and care plans — and that capacity-building funds can be used to buy equipment and address telehealth gaps. He said HCA would follow up to gather more data about telemedicine adoption and its clinical impact.
Nixon closed by stressing the program’s partnerships — with WASPC, DOC, DCYF, DBHR, MCOs, and local providers — and by noting the program’s public-facing materials and learning series to help facilities meet requirements. HCA will continue rapid-response oversight, TPA office hours and targeted technical assistance as more sites go live.
Next steps: HCA will continue onboarding cohorts and troubleshoot billing and EHR issues, report outcomes to the committee as facilities stabilize, and follow up with any committee questions about telemedicine use and site-specific barriers.