Lifetime Citizen Portal Access — AI Briefings, Alerts & Unlimited Follows
Hennepin Healthcare officials warn of mounting deficits, urge targeted state support and governance changes
Loading...
Summary
Hennepin Healthcare leaders told the committee that uncompensated care rose from $40M in 2020 to $104M in 2024, that about 75% of patients rely on public payers, and that the system needs short-term state support plus long-term payment redesign to avoid service losses and threats to statewide trauma and training capacity.
Hennepin Healthcare officials and the governor’s senior adviser on hospitals told the Health and Human Services Finance and Policy Committee on April 14 that the system faces substantial, immediate shortfalls and longer-term revenue shocks tied to federal policy changes.
Jan Malcolm, senior adviser to the governor on hospitals and health systems, described Hennepin County Medical Center (HCMC) as a statewide and regional safety-net asset and said recent, unusual events — including the closure of UCare and a major change in a national claims payment system — have intensified underlying structural problems. "Hennepin Healthcare and its flagship hospital, HCMC, play a critical statewide role," Malcolm said, adding that the committee should consider both short-term funding and broader payment redesign to preserve capacity.
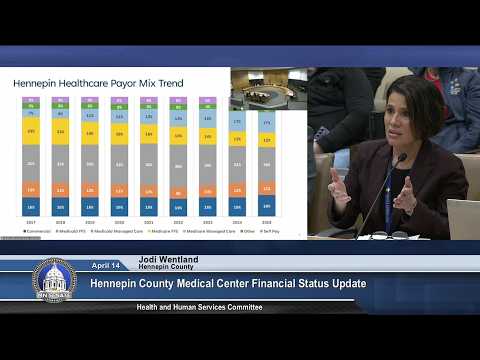
Jody Wendland, Hennepin County administrator, told the committee that uncompensated care at Hennepin Healthcare rose from $40 million in 2020 to $104 million in 2024. She said roughly 75% of patients rely on public payers (Medicaid and Medicare) and that, when combined with self-pay, more than 80% of patients lack a viable payment source, leaving the hospital with recurring operating losses and limited reserves.
Charles Esler, vice president of finance at Hennepin Healthcare, described the payer-mix shift and the loss of directed payments as a key driver of revenue loss: he estimated a revenue reduction on the order of $70 million annually compared with five years ago and presented a baseline annual operational shortfall of about $187 million. Esler said additional reductions tied to HR 1 could reduce revenue by approximately $1.7 billion statewide over 10 years and that directed payments would phase out incrementally beginning in 2028.
Joe Matthews, Hennepin County chief financial officer, reviewed capital and physical-plant needs: the campus is about 4 million square feet, much of it aging, and the county currently budgets $25–30 million annually just to keep buildings functional. Matthews noted an outstanding principal of roughly $131 million on existing specialty clinic debt and outlined a range of potential debt-support options ($80–160 million) to underwrite a larger campus investment if pursued.
Dr. Megan Walsh, chief academic officer and president of the medical staff at Hennepin Healthcare, cautioned that workforce instability threatens the hospital’s role as a level 1 adult and pediatric trauma center and its ability to train physicians. She said nearly 5% of the medical staff have resigned since January and that the loss of even a small number of essential specialists could jeopardize trauma accreditation.
Committee members asked for more granular counts and the underlying modeling (Esler said the statewide estimate of 140,000 people losing coverage was proportionally applied to HCMC in their analysis). Wendland said the county would post draft language for a funding proposal and provide a walk-through for the committee the following day. Members flagged the urgency: session time is limited and committee members pressed for both immediate, targeted funding and longer-term structural reforms.